
„The benefits of vertical positions include not only the help of gravity, but also shorter labour, more efficient uterine contractions, fewer operative labours, and fewer abnormal foetal cardiac findings.“
- David Desseauve at al. -
European Journal of Obstetrics & Gynecology and Reproductive Biology, 2017
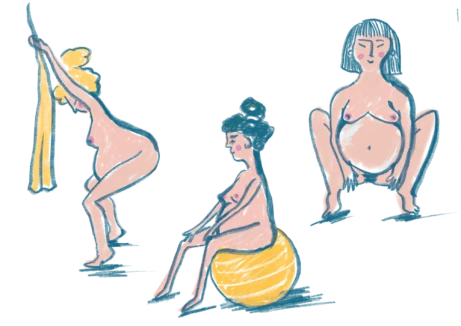
WHY Vertical positions?
We are used to seeing women give birth lying on their backs. And yet, it is more beneficial for mother and for baby to be mobile and upright during labour.
• walking • standing upright • standing with support • leaning forward • squatting • squatting and pulling on support • standing and pulling on support

• sitting on a birthing stool • sitting and leaning forward • kneeling and leaning forward • kneeling on all fours • kneeling on one knee • positions with partner
Active vertical positions support the natural biomechanics of labour.
„Walking and upright positions in the first stage of labour reduce the duration of labour, the risk of caesarean section, the need for an epidural, and do not appear to be associated with increased interventions or negative effects on maternal and infant well-being.“
- Annemarie Lawrence et al. -
Systematic review of 25 randomised and quasi-randomised trials from the Cochrane Pregnancy and Childbirth Group's Trials including data of more than 5000 women, 2013





Benefits of upright positions
WHY STAND UP FOR BIRTH ACCORDING TO EBM?
- pain intensity and stress levels
- risk of abnormal foetal heart rate
- risk of shoulder dystocia
- risk of acute caesarean section
- episiotomy rate
- need for forceps or vacuum extraction
- risk of severe perineal trauma
- need for synthetic oxytocin augmentation
- duration of all stages of labour
- positive birth experience, feeling of competence = lower risk of postpartum depression
- oxygen saturation of the foetus due to not compressing the vena cava inferior
- room for foetal rotation in the birth canal and positioning
- room for the coccyx to move
- contractions are more effective, more regular and stronger
- rate of cervical dilation
- ability to relax between contractions
- slightly more 2nd degree tearing in some sitting positions, but this is compensated for by a lower episiotomy rate
- higher risk of blood loss in sitting and squatting positions
- upright positions are also beneficial for women with epidural anaesthesia
„Giving birth is so much hard work and I have to stand and walk all day?“
„Not at all. Lean forward, hang onto something, swing, rock, put your weight on your partner. Move or rest as you please.“
„The routine use of the supine position during the second stage of labour should be considered to be an intervention in the natural course of labour and this intervention should be justified.“
- A. de Jonge et al. -
meta-analysis, 2004
Evidence based
Pregnancy simulation conditions of the computational model of the female pelvis resulted in greater increases in most pelvic measurements (predominantly at the outlet) in an upright birthing positions, especially in the final squatting position, up to 11.0 mm. Peak increases in diameter were demonstrated during the dynamic part of the movement, rather than the final resting position.
Flexible sacrum positions are associated with fewer episiotomies and higher chances for spontaneous vaginal birth. The findings are consistent with the current evidence suggesting that women should be encouraged to give birth in the position they feel most comfortable.
Childbirth requires the choice of optimal positions. These should be individualised for each woman at different stages of labour to improve its efficiency and effectiveness. Epidemiological data suggest that vertical birthing positions have many advantages. These include the use of gravity, shorter duration of labour, more effective uterine activity, lower rate of operative delivery, less abnormal foetal heart rate patterns.

“There is strong evidence that the second stage of labour should not be performed while the mother is in the supine position... Despite the proven advantages of giving birth in an upright position, most women deliver vaginally while lying on their back in lithotomy, semi-sitting, or semi-recumbent position. Because it is more convenient for health care providers to deliver in supine or semi-sitting positions, it is assumed that they are the ones who encourage mothers to give birth in these positions.” say the authors of a review of 42 relevant studies on birth positions about the importance of proper training for health care providers.
“Women should be encouraged to give birth in whatever position they find most comfortable.” states J. Gupta in the systematic review “Position in the second stage of labour for women without epidural anaesthesia”. Chosen positions have an impact on birth and on women's and children's health.
A systematic review and meta-analysis concludes that flexible sacrum positions in the second stage of labour may reduce the incidence of operative delivery, instrumental vaginal delivery, caesarean section, episiotomy, severe perineal trauma, severe pain and shorten the duration of active pushing phase in the second stage of labour. Only 2 of 12 studies found an incidence of severe perineal trauma suggesting that flexible sacrum positions reduce the relative risk of SPT by up to 75%.

Walking and upright positions in the first stage of labour reduce the duration of labour, the risk of caesarean section, the need for an epidural, and do not appear to be associated with increased interventions or negative effects on maternal and infant well-being.
Healthcare providers should encourage the adoption of a birthing position of individual choice during the first and second stages of labour, including upright positions, even if women have epidural analgesia.
Upright and lateral positions have more potential benefits in improving maternal and neonatal outcomes and managing with certain obstetric complications. However certain upright positions such as squatting position and sitting position, may correlate with perineal trauma and increased blood loss. Lithotomy and supine positions should be avoided because of the possible increased risk of severe perineal trauma, comparatively longer labour, more pain, and more foetal heart rate patterns. So say the authors of the review and comparison of the benefits and risks of common maternal positions during the second stage of labour, to provide evidence-based practical guidelines for midwives. Based on 70 relevant sources (studies, metastudies, systematic reviews, trials etc.)
A Swedish cohort study of 12,782 women suggests that midwives should be aware of their influence and encourage women to choose upright birth positions. The study suggests that the choice of birth position may be determined more by midwives than by women's preferences. Despite being randomised, women who gave birth on the birthing stool were statistically significantly more likely to report that they participated in decision making and that they took the opportunity to choose their preferred birth position. They were also statistically significantly more likely to report feeling strong, protected and confident. And they were more likely to report less pain and a positive birth experience.
How we take care of women during labour, and the psychosocial environment in which labour takes place, is important and has an impact on women's mental health. Companionship and support modifies factors that contribute to the development of postnatal depression.
Vertical positions are instinctive. The majority (65.2 %) of 3000 women in the cohort study used upright flexible sacrum positions. However, the position assumed by women during labour is influenced by several complex factors. Upright birth positions occur more often within certain birth settings, such as birth centres and homes. The midwife’s preference as well as cultural values may influence the position for birth.
A population-based prospective cohort study of planned home births in four Nordic countries between 2008 and 2013.

“The routine use of the supine position during the second stage of labour should be considered to be an intervention in the natural course of labour and this intervention should be justified.”
Upright positions in the second stage of labour are also beneficial for women with an epidural.


#GOatout campaign:
Why are there goats all over this PAGE?
Goat is a slang term for the birthing bed in Czech. Not because it is the Greatest Of All Time, but because the stirrups look a bit like goats horns. Therefore the slogan: Goat out!
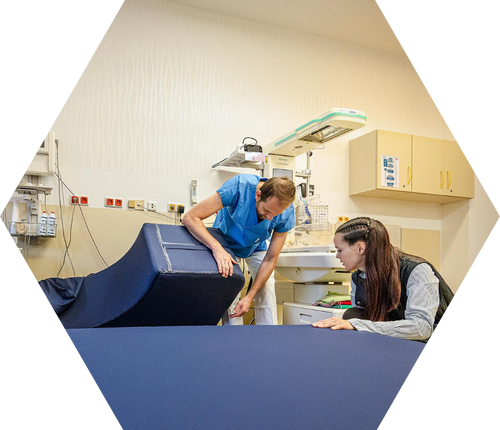
Since October 2023, Propolis33 has been helping Czech and Slovak hospitals enhance their birthing suites by replacing the birthing bed with a birthing couch in an effort to create an "environment that supports physiological birth" for healthy women. In cooperation with UH Ostrava they lauched an educational campaign to inform about the benefits of active vertical birth. Within the first year, over half of all Czech maternity hospitals came on board aquiring a birthing couch.
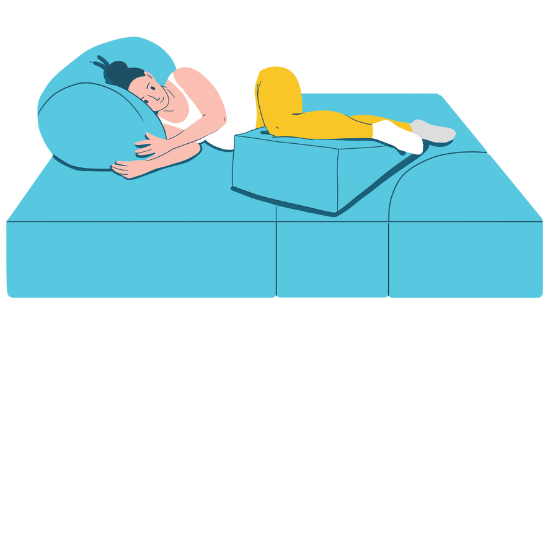
Labour room equipment
This is important. The birthing bed (“goat”) in the middle of the room automatically encourages one to lie down. Birthing couch, stools, hanging slings and various supports to lean on encourage one to move around and be in vertical positions. Maternity rooms equipment affects the way women give birth there.
COMFORT AND PRACTICALITY = SMOOTH BIRTHING PROCESS
- birthing stool
- slings to hang on to
- gym balls, bean bags
- birthing couch / simple hospital bed
- obstetric bed within reach in case of complications (in the corridor, in the storeroom, or in the corner of the room behind a curtain, simply out of sight)
„What do we need? For both mother and medical staff to be as comfortable as possible.“

Woman giving birth: Lucia Kalcikova / @luciagenethad / @dulapetraskalska / @moni_porodni_asistentka / @pav_m_photo
“The couch is much more convenient for medical staff than mats on the floor. That is very important, since midwives who spend many working hours in delivery rooms need to keep themselves healthy.”
“An easy way to encourage the father to actively participate during labour and the possibility of uninterrupted bonding of the whole family immediately after birth opens new chapters in hospital care. It feels like giving birth at home.”
“We gave birth to our second daughter Eliška on the birthing couch. It was wonderful, very comfortable. I was on all four and my husband was able to support me all the time.”





#goatout and couch in!
“We felt at home. We were one of the first couples who had the opportunity to give birth on the birthing couch, so it was possible to be together the whole time. It was such an incredibly powerful experience. The moment when the doctor placed the newly born Larinka on my wife's chest is something I'm going to remember forever.”
– Martin and Simona, parents, MU Litomerice, 2023
Obstetric birthing bed
- Offers variability and many different settings with handles and arms allowing for various positions. Is designed to provide easy access and good visibility for medical procedures in case of complications.
- It is complicated to change settings, the position is higher, which restricts woman's natural movement between bed and floor, leads to preference for semi-supine and other horizontal positions and implies a passive role for the mother.
Birthing couch
- Simplicity, light weight, offers variability, quick changes of shape and ways of support, adjustment and use is intuitive and simple for women and caregivers, low enough for women, high enough for staff, natural involvement of partner/support person, the whole family is together from the first minute on - plenty of space for family bonding postpartum, encourages mobility in vertical positions, encourages the use of various positions - forward leaning, lying on the side, swinging etc. as well as an easy change of position, mother as the central figure.
- Doesn't have handles, it is recommended to attach handles or railing on the wall, is not suitable for the treatment of some complications.
"My first birth was on a "goat", and although everything went well, I still have terrible memories of pushing while lying on my back. My second birth was on the couch, it was amazing, I especially loved rocking on that swinging piece. My only regret is that the change did not come sooner."
Where can you buy birthing couches?


Ondrej Simetka
ObGyn consultant, Head of ObGyn Dept, University Hospital Ostrava, CZ
How are birth injuries treated on the couch?
How is excessive bleeding dealt with on the couch?
How is the couch cleaned and disinfected?

Is the couch comfortable enough for the staff?
"Choosing their position during childbirth at their own discretion empowers women. It boosts their self-esteem. The feeling that they are not "puppets" of medical staff, but autonomous beings who have brought their child into the world according to their own wishes. This helps make a positive birthing experience and a woman proud.”
BIRTHING COUCHES IN CZECH REPUBLIC and Slovakia
The following hospitals in the Czech Republic and Slovakia have acquired both a birthing couch and underwent our implementation workshop on active vertical birth and practical couch care guidance:
SK: Trenčín, Trnava, Stará Ľubovňa
BIRTH COUCHES may also be found in the following hospitals:
SK: Prešov, Zvolen
BIRTHING COUCHES at the faculties of midwifery studies








WHAT DOES OUR IMPLEMENTATION WORKSHOP CONSIST OF?
Thanks to Propolis 33 endowment fund we can offer free training workshops to MotherBaby-friendly maternity units. The training is a 2 to 3 hour long workshop, which includes a theoretical and a practical part. We provide the historical context of the development of birthing positions and the modern scientific debate; discuss which positions support the physiology of the birthing process; compare obstetric birthing beds and birthing couches, including why and how a couch can support a woman in her mobility and verticality during labour. We also pay attention to the role of the midwife and other medical staff, ways in which the husband and doula can be involved and the practical aspects of working with the couch - maintenance and care. We always work as a team of a doula and a midwife or ob/gyn.Founder of Propolis33 endowment fund

"Cultures from Africa, Americas, Asia, Europe and beyond - the same upright positions prevail everywhere. History corroborates the evidence of ethnologists that points to the prevalent use of upright positions in childbirth throughout the ages."





”When I researched ethnographic sources about labour in Southeast Asia and Melanesia, none of them included the supine position. And there were dozens of cultures. Positions used were always sitting, squatting or on all fours. Women were often leaning against a pillar or hanging onto something. The supine position has benefits for medical staff and institutions, but it does not make sense for the active protagonists in this process - for the woman and baby.”
- martin soukup -
anthropologist

I was surprised at how easy it was to replace the medical birthing beds with birthing couches and how well it was received by staff and parents.
Advantages include its variability, better support in many positions, more active involvement of the mother and the partner, and the possibility of resting together after birth. Third couch is on its way. Satisfaction prevails. You can read the exact statistics from UH Ostrava here.
- Ondřej Šimetka -
ObGyn consultant, Head of ObGyn Dept, University Hospital Ostrava, CZ
Active labour means that the woman is free to move as she wishes and can follow the needs of her own body.
I studied with Janet Balaskas, the author of 'active birth', which changed birthing positions in the UK and around the world. The key point is for the woman to get up from lying on her back. What matters is a woman's freedom to choose her position in labour. I see great potential in how a birthing couch can help achieve this, which is why Propolis33 has been involved from the start in the campaign to bring birthing couches into Czech and Slovak maternity wards.
- Lilia Khousnoutdinova -
Founder of Propolis33 endowment fund

Propolis33 endowment fund:
Peer review:
- Magdalena EzrovAPresident of the Union of Midwives UNIPA Member of the Midwifery Commission
Consultant:
- Ondrej simetkaHead of ObGyn Dept, University Hospital Ostrava, CZ
- Peter KaščákHead of ObGyn Dept, University Hospital Trenčín, SK
Endorsed by: